ia801708.us.archive.org/6/items/sreyas-ebooks/sreenarayaneeyam-vyakhyanam.pdf
Narayaneeyam
Dr Bhavani Chandrasekharan’s Blog
Gives articles based on career(doctor)experience
Did You Know?……..About Uterus Transplantation
————————————————————————-
Did you know that just like kidney,liver and heart,UTERUS also can be transplanted to a woman’s body?
Did you know that pregnancy can grow and develop almost upto term in the transplanted uterus and a live and healthy baby can be born?
Yes.Uterus Transplantation has become a reality in many parts of the world including India.India and a few other countries have been successful in growing pregnancies in the transplanted uteri and bringing out healthy babies.
Mothers can donate their uteri to their daughters.Siblings,relatives,friends or any ladies in that order,can be uterus donors.
Please note that it just cannot be plucked like a flower from the donor and clipped into the recipient’s body.Just like any other organ transplantation a series of tests are to be conducted on the donor and recipient so that the recipient’s body does not reject the new uterus.How meticulous the tests and checkups may be,a good percentage of rejection chances are there.Immunosuppressant (anti rejection)medicines are given in the necessary dosage to minimise rejection chances.
The surgery on the donor as well as the recipient are really complex and the surgeons and their teams should have very precise expertise and dedication.It is a 6 to 12 hours of intense work.It is not just the uterus,but adjacent parts like a cuff of vagina,blood vessels etc are to be removed from the donor without injuring parts like urinary bladder and ureters.Otherwise the donor will have to face major postoperative complications.If the donor is a dead woman the operating time and difficulty on the donor is less.The parts are to be sutured perfectly in place in the recipient.If signs of rejection become obvious,the transplanted uterus has to be removed immediately.Thus the very expensive procedure can go in vain.
Once the transplanted uterus shows normal functioning,pregnancy is attempted by assisted reproductive techniques like IVF((In Vitro Fertilisation).Here sperm from male and egg from female are made to unite in a dish(test tube) and the embryo is implanted into the uterus.IVF too is not as simple as it is said.It is expensive and successful to the maximum of 40% only.Pregnancy by IVF, in a transplanted uterus,in a lady who is on anti rejection drugs,faces more chances for anomalies.Delivery is always by Caesarean section.
After one or two deliveries the transplanted uterus has to be removed so that the immunosuppressant drugs can be stopped.Apart from their cost,they act by suppressing the body’s own immune system which tries to reject the transplanted uterus.If the immune system is suppressed,the body gets victimised to various illnesses.
Transplants like liver,kidney and heart are life-saving.Though the recipient needs life-long anti rejection drugs,with proper care,he can get many more years of healthy and comfortable life .But in the case of uterus transplant,it is never a lifesaver.The recipient lady can be happy about having a functioning uterus to the extent of bearing a child of her own,at the expense of a series of complex procedures.
Anyway its a great research work globally and the doctors and their teams need to be congratulated and honoured immensely.Let us be proud of India’s such Health Research Programmes and their implementation.
PHOTO—–INDIA’S FIRST UTERINE TRANSPLANT BABY

GAS TROUBLE-GERD
———————————
Old trouble with new name!! ‘Dr,will you write on GERD?I suffer just that’....a friendly request reached me once.My friend didn’t meet a doc.Google was her homely inexpensive consultant.Like any other of my fraternity I too got irritated with such patients but of late I started taking advantage of the Google-provided awareness of my patients to the extent that I asked them to ‘google out’ more details of their concerns before their next visit with a warning of course that Google should never treat them.
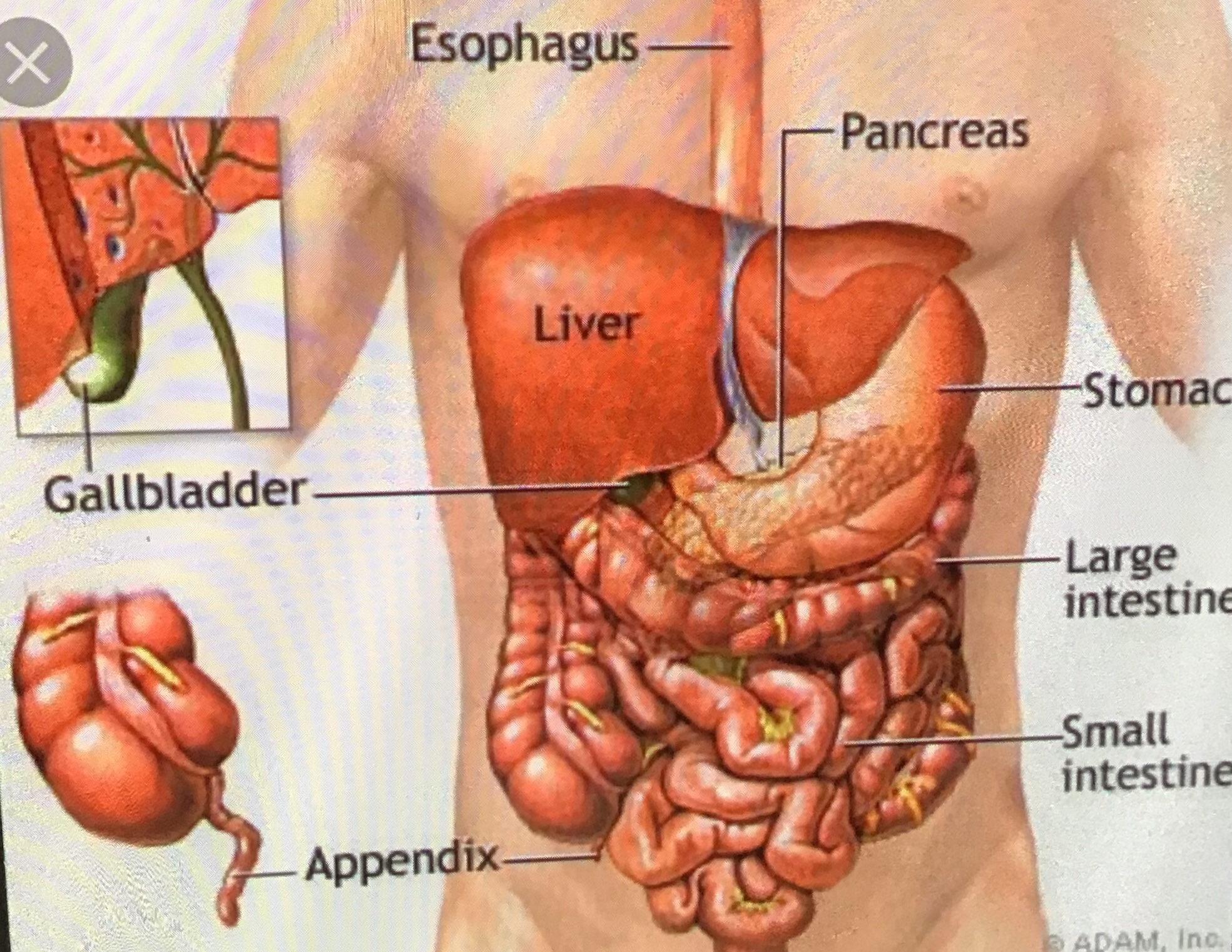
Yes,our good old gas trouble is now branded as GERD-Gastro Esophageal Reflux Disease.Gastro means stomach,Esophagus means food pipe which extends from throat to upper part of stomach,and Reflux is back flow.
The food we take,mixed with saliva- the watery mouth secretion,is gulped via throat into the food pipe.It reaches the stomach in about half an hour.There is a circular muscle around the lower end of the food pipe(Lower Esophageal Sphincter-LES).This muscle opens for the food to pass from the food pipe to the stomach and closes. Normally LES never allows backflow of food or other stomach contents like acid and bile into the food pipe.(Stomach acid is produced in the stomach itself.Bile is the fluid secreted by liver,stored in gall bladder and released into the upper part of intestine.These are needed for digestion).
If LES is weak or malfunctioning,the backflow (reflux) happens.This exactly is GERD.Sometimes a small part of stomach gets herniated into the chest.This gets aggravated with cough,strain,full stomach or pregnancy.This is called Hiatus Hernia and this also weakens the LES.
Do you get acid(sour)burps?
Does the middle of your chest burn?(heartburn)
Does your chest ,mostly the middle part, ache?
The ache does not aggravate with exercise and
does not subside with rest?
Something rolls up from upper tummy to throat?
Something obstructs your throat?
You have a food-coming back to mouth feeling?
You feel like vomiting or you just vomit?
You feel very uncomfortable after a full meal,more
so if it is spicy/sour/fried/non veg?
You feel heartburn and nausea when you are
stressed?
You cough frequently without cold or respiratory
infection?Your asthma is worsened?
No doubt,need not google,you have GERD.The symptoms may occur twice or thrice a week,sometimes more frequent,may last for weeks and subside self and reappear soon.A Physician is to be consulted who may refer you to a Gastroenterologist.
As do many other diseases,GERD too is kept away by proper lifestyle and foodstyle.
Obesity is the result of unhealthy food ,overeating and sedentary life.GERD is very common in the obese.So proper weight maintenance important.
Avoid eating to the full stomach.Small frequent feeds are ideal to avoid the nasty backflow.Do not relax while in full stomach.Have supper at least 2hours before you go to bed.Avoid spicy and fried food to some extent at least in the day to day life.Avoid them in a big way if you already have indigestion due to GERD.Try to keep food timings as far as possible.
Coffee,chocolates,pepper,citrus fruits like orange and lime; alcohol and tobacco add to the reflux and better keep them away.
Medications with painkillers,aspirin etc worsens GERD.
Tense hard work neglecting food adds fuel to fire.Mental calmness at home,workplace and outside keeps away the gas trouble in a big way.Proper sleep is essential.Calm and clear mind only can provide good sleep.
Head end of the bed kept raised by 6 inches with a suitable block gives good relief of symptoms.Upright position always gives a lighter feeling.
GERD is very common in pregnancy.Pregnant women are advised easily digestible food which is taken frequently in smaller quantities than usual.
Even in infants and children who often refuse food,let out burps and hiccups,vomit or cough or cry incessantly,and are irritated while feeding , GERD is diagnosed.
Antacid liquids and tablets like Gelusil and Digene neutralise the acid that backflows to the foodpipe.Some antacids contain a foaming agent that forms a foamy layer along the inside of the foodpipe.Some have a local anaesthetic to reduce pain.There are other medicines like Ranitidine and Cimetidine which reduce the production of stomach acid .Pantoprazole,Omeprazole,Lansoprezole etc are medicines that block the acid production and allow healing of the foodpipe.Domperidone helps to subside vomiting sensation.
If symptoms do not subside with life style and food style changes and the usual medicines,doctors do tests.
The main test is endoscopy.A thin flexible tube fitted with light and camera is passed through the foodpipe to see the inside of it and the upper part of stomach.Biopsy can be taken from a suspected part if needed.
There are tests by which the doctor can visualise the upper part of intestines also.
There are tests to detect the acid level in the foodpipe and upper part of stomach.
Test to measure the strength of muscles especially the LES ,is available.
Another test measures the movement of substances in the foodpipe.
If medicines fail to heal the ulcers,very rarely the doctor thinks of surgery.
Fundoplication is a form of surgery where the upper part of stomach is stitched like a cuff to the lower end of the foodpipe to strengthen the LES.
Electrodes are used via endoscopy to promote scarring on the LES and strengthen it.
Too much of acid inside the foodpipe can damage its lining causing infections and ulcers.Ulcers can cause bleeding.Ulcers heal by scarring and narrowing (stricture) of the foodpipe can happen.Some ulcers can be precancerous.
GERD can aggravate asthma , tooth infection and gum disorders.
Anyway apart from the” trouble “ one suffers,GERD is never life-threatening.

A Rare Labour room Emergency
———————————————-
Labour room is the most important work arena of a Gynaecologist.Labour pain is the hardest form of pain a lady is destined to suffer.In this era of ‘painless labour’ many in our country still do not opt for that.Of course the pain duration is much lessened with safe medicines.
Loud hues and cries,angry and even abusive words,big or subdued sobs,attacks with hands and feet..what all actions from ladies in labour we face there!!The lady who enters the labour room smiling and calm,sheds all her inhibitions and gradually adopts a different behavioural pattern when the pain threshold is lost. Of course she is in happy tears and smiles of gratitude once she perceives her baby’s soft sweet cry.
With all these din and bustle how I loved my labour rooms!!The floor always bore stinky stains of blood and other body fluids though cleaned instantly.A Gynaecologist can be successful only if she likes the labourroom atmosphere.Watching expressions of the new moms and their bystanders on seeing the newborns used to enchant me immensely.
99% ladies are happy and easily forget the pain part of the great event once they and their newborns are marked safe. I have to mention that a few of them are taken up for Caesarean deliveries as a safety precaution.Very few nurture the memories of pain and refuse to conceive a second time.Please note that the second and subsequent ones are less and less troublesome,a painless labour can be opted also.
Labour room is a place where sudden and startling complications can ensue for any healthy lady.A Gynaecologist has to be available 24/7 and is to have the expertise and presence of mind to handle such unpredictable situations successfully.
Bleeding during and after deliveries is the common major problem we face.It can happen all of a sudden on any lady and we have to anticipate and be prepared to face same.Availability of enough blood/blood components/other paraphernalia is to be confirmed regularly.The most difficult part is to convince the bystanders about the unexpected complications.They often consider the healthcare providers as culprits.Fortunately this part was nice for me as my patient folks always understood the situation and supported me with prayers.
My meeting with Mrs C yesterday in a wedding ceremony prompted this storyline.2decades back she saw me for her first pregnancy.This 23 yr old beautiful,smart,blooming and energetic patient-friend entered my labour room one fine morning with mild pains and joyful expectations.There was no need for tender touches and consolations as she was nice to say she would suffer any pain for her baby,and she kept her word.She let out her healthy bundle of joy into my hands soon.Every newborn made me happy as though it was a first baby through my hands.
It was a rather busy labour room that day with 5,6 more deliveries ahead and fresh cases keeping on entering.Entrusting the expulsion of Mrs C’s placenta with my experienced assistant I got busy with the next patient in the adjacent cot.
My assistant called me in panic to see Mrs C.The placenta had separated 30minutes after delivery only(long but acceptable interval) but the uterus had turned upside down,the uppermost part (fundus) of the uterus could be seen big outside with very profuse bleeding and Mrs C was going in for a ‘shock’.Her BP came very low,pulse was very rapid,the body was cold and sweaty,she vomited and was semiconscious…ACUTE INVERSION OF THE UTERUS had happened..the rarest of rare incident.
I had seen only one case in the labour room of Calicut Medical College and I remembered how panicky our HOD,Professor T,was then.The patient ,who had her 7th delivery,did not survive.She was in shock and she bled to death.Yes,Acute Inversion can cause death within a very short time if not interfered very promptly with all the supportive measures sufficient and handy.The only case I had witnessed was in 1973 and the case of Mrs C was in 1997…we were better equipped.
I tried my level best to hide my tension.I tried to keep back the uterus in position while hasty preparations were being made for a surgery.My attempt was a failure as a tight band had already formed around and above the big protruding part of the uterus.
The General Surgeon was summoned who said he knew very minimal about such a case.I asked him,a person who could use a surgical scalpel very effectively as per instructions,to be with me.A briefing about the grave situation was done to the bystanders.
On the table Mrs C lay virtually lifeless and extremely pale. My Anaesthesiologist asked me to concentrate on the surgery without seeing the very bad numbers on the monitor.
Nothing was there in the tummy in place for the uterus.It had inverted fully and gone down.No time to lose,memorising the textbook description of Haultain’s manoeuvre I made an incision in the midline at the back of the tight ring that had formed on top of the inverted uterus and gradually pulled it up to the normal position and stitched up the cut part.With unit after unit of blood and other measures already on,Mrs C’s condition improved dramatically and she was discharged home after a week.She had two Caesarean deliveries later and the uterus never showed any signs of the past insult on it.
This can happen to any patient in the labour room.Causes cited are weak and thin uterus after repeated deliveries or abortions,placenta implanted at the topmost part of uterus (fundus),wrong and impatient way of pulling the umbilical cord to deliver the placenta,and NO SPECIFIC REASON.Mrs C’s case fitted into the last category.
I explained to her well about Acute Invertion of uterus and how she happened to be my first patient with that problem.Later whenever we met she rushed to me to know if I had another similar case.Till date she is very proud that she was my sole case of inversion!!

DIALYSIS
————-
10yr olds even know about ‘dialysis’ nowadays.Somebody in their household or neighbourhood must be undergoing this treatment which has become so common and so handy to sustain prolonged life for kidney failure patients.Before the advent of dialysis and kidney transplant,kidney failure led to death for sure.Nephrology (science related to kidney related problems)service including dialysis facilities are available in all major private and govt hospitals.There are independent dialysis centres also.Dialysis team can help in home dialysis.Many hospitals offer charity services to deserving patients.
When we consume food and drinks,our body uses what is needed and the rest is turned into waste products and excreted as urine by our healthy kidneys.They also help in production of red blood cells and prevention of anemia .They activate vitamin D to maintain calcium levels and bone health.They regulate blood pressure.They maintain body’s fluid balance.Chemicals like potassium,sodium and bicarbonate are kept in safe levels by them.When kidneys fail to work waste products accumulate in our blood and cause all complications leading to death finally.
Dialysis creates an ‘artificial kidney’ in a patient whose kidneys have lost 85 to 90% function.His GFR(Glomerular Filtration Rate)which should have been 90%or more, is less than 15. (Glomeruli are units inside the kidneys which filter out waste from blood).
GFR is a calculation from the results of the patient’s blood creatinine test,age,weight and gender.
GFR is an unfamiliar word but ‘creatinine’ is nowadays as famous as ‘cholesterol’.The first ‘c’ has overtaken the second ‘c’ actually!!
But what’s creatinine?How’s it connected with kidney function?
Our muscles contain a product called creatine phosphate.Creatinine is produced from this creatine phosphate.It is a waste which is removed from our blood by kidneys regularly.If kidneys fail,creatinine level in blood gets elevated.
Normal creatinine levels are 0.6 to 1.2 milligrams per decilitre in males and 0.5 to 1.1 in females.As age increases the level goes a bit higher.In obese persons also it is seen slightly high though kidneys function normally.
Significant amounts of blood and ‘albumin’ are let out in urine by damaged kidneys.This can be detected by a simple urine test.
Various scans of the kidneys are suggested by the Nephrologists.A biopsy may be taken.These tests show if the kidneys are bigger or smaller,and if there are stones,infections and cancer.They also show the extent of damage that has happened to the kidneys.
A patient with kidney failure can have symptoms like nausea,vomiting,tiredness,giddiness,swelling especially on ankles,less urine,blood pressure variations etc.Sometimes he will not have any symptoms at all.Importance of health check ups has to be emphasised here.
Associated conditions like Diabetes,high blood pressure,liver problems and obesity enhance kidney
failure.Self medications especially with pain medicines can result in kidney damage.
Please get treated by qualified doctors only,not only in Allopathy,but also in Ayurveda,Homeopathy etc.
Kidneys can fail suddenly (acute)as a complication of infections like viral fever,accidents,blood loss,heart and liver diseases,medicines,severe burns,severe allergies,severe dehydration,complicated surgeries,poisoning etc.
Gradual kidney failure(chronic) is due to diabetes,high blood pressure,polycystic kidneys(genetic,can run in families),inflammation of kidneys (nephritis),auto immune diseases(our disease fighting mechanism is affected),improper use of medicines and many unknown causes.
Both acute and chronic kidney failures are dangerous for life.Acute condition needs very prompt treatment,mostly with dialysis but subsides with a few courses usually.Chronic kidney disease needs lifelong treatment ,mostly with dialysis and the Nephrologists may advise kidney transplant.
Dialysis is mainly of 2 types-Peritoneal Dialysis and Hemodialysis.
Peritoneum is a thin membrane that lines the interior of the belly as well as wraps the organs inside it.In ‘peritoneal dialysis’ the peritoneum is made to act as natural filter to remove waste from our body.
‘Hemo’ means something connected with blood.In hemodialysis a ‘hemodialiser’ is used to remove waste from the patient’s blood .In the arm or leg an artery and a vein are joined together to form a ‘fistula’.Through this portal the dialiser is connected. Sometimes,in emergencies,a neck vein is used for dialysis.
Diet is very important in patients with kidney failure.
No extra salt is added to food.Very salty processed food items do great harm.Less salt is always a kidney-friendly way.
Unused protein from our food is broken down to waste products such as urea and creatinine which are eliminated by our kidneys.If kidneys fail,these wastes accumulate.Eating large amounts of protein food like meat,fish,chicken,eggs and dairy products make matters worse naturally.But once dialysis treatment has started,sufficient proteins will be advised by the doctor whose advice is to be followed strictly.
Phosphate is a mineral found in meat,dairy,nuts and cola.Calcium and phosphate keep our bones,teeth and blood vessels healthy.In cases of kidney failure excess calcium and phosphate accumulate in blood and form hard deposits in heart,lungs,blood vessels,joints etc.Bones also become brittle,painful and break.So such phosphate rich foods are to be cut short as per the doctor’s advice.
Potassium is a mineral good for muscle strength.But high levels affect heart rhythm.In kidney failure if potassium level is to be maintained ,we should avoid bananas,dried fruits,peas,beans,spinach and potato.As said before,once dialysis works in the right way,doctor will advise you about adding these much useful items in your food menu.Tender coconut water too is rich in potassium.
Patients on dialysis should strictly follow fluid restriction advice.This mainly depends on the quantity of urine produced daily.Fluid overload can be dangerous.Dehydration also is harmful.Salt restriction makes one less thirsty.
Dialysis needed or not,which type of dialysis,how many times a week,tests before and after,at home or hospital,diet schedule,activities,treatment of associated diseases,treatment of dialysis-related complications if any ,need for a kidney transplant..all these will be decided by a Nephrologist and his team and discussed with the patient in detail.Every patient is different from every other patient.Possible dialysis-complications are blood pressure variations,muscle cramps,nausea,vomiting,itching,sleep problems,pricking sensation in legs,anemia, bone diseases and fluid overload.
Average life expectancy on dialysis is 5 to 10 yrs but patients have lived upto 30 yrs even.This depends on our other medical conditions.Strict adherence to the Nephrologist’s instructions is extremely important.

A faulty deed rectified
———————————
We were proceeding to the footwear stand after a blissful worship at Thodupuzha Krishnaswami Temple.Mrs V whom I had met inside,was waiting for me there.She made the sandal paste mark(Prasadam) on my forehead more perfect wiping the extra portions with her hand and slipped in a piece of plantain cutting with butter(again Krishna’s Prasadam)between my lips.Moving to my back she pulled down gently the lowest portion of my saree to hide my heels.I was not surprised as I am used to such concerned gestures from her wherever we meet,absolutely no inhibitions for her.
She must be 44 now as her son now is 26,finished his MBA from a reputed institution and well placed job wise.
V came to see me with her mother 26 yrs back with complaints of irregular periods,no periods at all for many months,obesity,thyroid problem,abnormal hair growth,increased appetite etc.She was doing her 1st year B.Com in the local Govt college.She was very obese I noted.
I was shocked to find a 20 weeks size pregnancy in her.She and her mother looked perplexed and totally denied a chance for pregnancy in the unmarried V.I could extract the fact from the girl that she never expected pregnancy though her neighbourhood family friend/long time classmate boy had bodily contact with her just once,sometime back.
The boy owned it up anyway but his parents were adamant that the pregnancy should be terminated and they could marry later.
I knew both families and explained that legal termination is not possible after 20 weeks,and termination can be dangerous as no qualified doctor would do that.I insisted that the boy and girl should marry immediately as just 4 more months were to go for her delivery date.They planned a register marriage but I told them to conduct a wedding celebration inviting as many natives and relatives as possible.A delivery after 4 months would be better accepted by the public that way than a hushed type of register marriage.
I knew they had knocked at many doors to get a termination of pregnancy done but in vain,no doc helped them.Finally I got the wedding invitation!!
They have a happily bonded life till date.The 26 yr old young man has a younger sister also.He knows his parents’ love story .He knows me also.I ask him in a lighter vein…”any  girlfriend in the neighbourhood,pregnant?”..He says smiling,”no ma’m,it won’t happen”..
girlfriend in the neighbourhood,pregnant?”..He says smiling,”no ma’m,it won’t happen”..
SHE IS ALIVE!!
———————
Mrs X at 31 yrs,was happily pregnant with her second child.The first scan at 6weeks’ pregnancy time showed no evidence of a pregnancy inside the uterus.I always nurture in my mind a caution in such cases.it can be an ectopic pregnancy,ie,a pregnancy in a location other than inside the uterus,for example a tubal pregnancy.Pregnancy of Unknown Location (PUL) is always a matter of concern as it cannot grow beyond a particular stage and will terminate in a life-threatening way.
Mrs X was advised in the right way and she turned up for a second scan 2 weeks later.Both of us were happy and relieved to find a live pregnancy inside her uterus itself.She was very obese and had a lot of hormonal problems naturally.
Exactly one month later,one day nearing her check up date,she landed in our Emergency Care Unit at 10 pm with a sort of lower abdomen discomfort and nausea.She always had gastric upsets before also.A pregnancy scan was done to see a healthy baby inside,though I felt it was implanted more on the right corner of the upper part of the uterus where the Fallopian tube opened.
At midnight she developed a sudden severe pain,vomited and became semiconscious.Her pulse and respiration were too rapid,her blood pressure too low,her body cold and sweating and the tummy got distended more and more.She was in ’shock’ due to internal bleeding.The pregnancy location near the right corner struck my mind.A part might have been implanted in the narrowest part of the right Fallopian tube which opens into the uterus and this part might have ruptured causing very profuse bleeding from the side of the uterus.
SHE WAS DYING WITH INTERNAL BLEEDING.All her vital organs were failing due to lack of blood circulation.All her blood was pouring fast into her abdominal cavity .Her Haemoglobin was just 4 grams/dl.This was 12 grams/dl at 10PM..so grave was the situation.
Absolutely no moment to lose,emergency arrangements for blood and medicines were done.Other specialists and staff were summoned to the theatre.Bystanders were informed briefly and consent was got for any lifesaving procedure.My Rev.Sisters started their prayers in the chapel.
Our Anaesthesiologist was struggling to keep Mrs X alive with intubation and oxygen,intravenous fluids,medicines like adrenaline,dopamine etc,blood (7 units were already available) and blood substitutes.He was watching the monitor in dismay and and asking me silently to proceed very fast.
Yes,I could reach the abdominal cavity within minutes,rapidly suck out the litres of blood inside,reach the right upper part of the uterus from the pool of blood without seeing it and pull it up to see a big rupture there with very profusely bleeding blood vessels.The pregnancy with the 3 months grown baby had slipped into the abdominal cavity.The Fallopian tube had been detached and hanging free pouring blood.
There was no meaning in retaining such a damaged uterus and it was removed fast.Fortunately she had a son delivered by me 10 years back.The husband in the Middle East was not willing for the uterus removal but could convince him over phone which was glued to my ear by a nurse.
The bleeding stopped,the lost blood replaced and the hurting organ removed,resulting in regaining a precious life.The kidneys ,heart,lungs and other organs restarted their functions happily.
Reason for such a calamity,very rare indeed, may be asked.A block in the Fallopian tube very close to the uterus might have happened,preventing the embryo formed in the tube from moving in and getting implanted well inside the uterus.It might have got stuck by a small part in the tube and the major part inside the uterus.So growth upto 3 months was possible.This cannot be easily detected by a Sonologist(one who does the scan).Mrs X had mentioned about a lot of infertility tests she had undergone while in the Middle East,like tube testings,D&Cs,Laparoscopy etc.Not that such tests are bad,but slightest infections inherent in such procedures even can cause scarring and tubal blocks.
Last night I was called just to support as an onlooker for a similar case,which prompted me to write this article.The patient was saved too from the gravest calamity by our rapid and expert action.

Courtesy..Dr Shimna Azeez
Varicose veins are big,dilated,entangled and curled blood vessels.
“We need only garlic,orange juice and olive oil to
‘cure’ varicose veins”..were you confronted with such a video message in WhatsApp yesterday?This message was shared 30,000 plus times in Facebook at a jet speed!!! Many were lamenting,”How sad!The season for oranges has ceased.Cannot try the remedy now”.Friends,don’t get upset.You are accorded a cordial welcome here.
We know our heart is a pump that reaches blood to all our body parts.Arteries are the blood vessels that take pure oxygen-rich blood to the trillions and trillions of cells in our body. Veins are thinner blood vessels that take impure blood from all over the body to the heart.A fourth standard student knows these simple facts.Hence no need for assertions but our video maker asserts that arteries take blood from the body parts to the heart!!The series of blunders starts with this statement.
Varicose veins are usually seen on the calf(back part of the leg below knee).Inability of the calf muscles to pump up the impure blood to the heart leads to pooling of blood inside the veins there.Pressure inside the veins raises and loosens the valves inside. The veins distend much with blood,thin out, curl like worms and entangle to show up as bluish soft raised parts along the leg.Prolonged standing or sitting in the same posture,obesity, aging and pregnancy are the main reasons.It is more in women who have had repeated pregnancies.Heredity has a definite role too.
It is quite unscientific to state that massaging garlic and orange paste twice daily on varicose veins can cure the problem.The video says:”Garlic is a magic medicine which can purify blood”.Though true that garlic has some medicinal value it is a big folly to believe that the externally applied paste can correct structural disorders like varicose veins.
It is better to avoid prolonged standing and sitting in the same posture.Do active exercises for half an hour at least for five days a week.Body weight has to be maintained with healthy foodstyle.
Treatment need not be initiated as soon as those blue veins are seen there.If there is associated pain,discomfort,itching,swelling,ulcer or bleeding,one has to consult a General Surgeon who may direct to other super specialists as and when needed.
Wearing stockings and doing exercises only are needed initially.If no relief there are procedures like surgery just underneath the skin,sclerotherapy (injection of medicine into the veins which makes them shrink)and laser treatment as other options.
If planning to opt for other systems of medicine please take care to see qualified doctors only in the concerned system.Please don’t pledge your health and wealth to fake doctors.
Be aware that there can be side effects to the ‘magic remedies’ also.At this instance I remember a father who hurt his child by applying smashed garlic overnight on a wart(a small harmless raised skin protrusion)on her leg.I saw a big blister on that part which looked like burns.I prescribed medicines for healing the wound.The father was very shrewd in asking me-“Doctor,hope there won’t be any side effect for these medicines”!! I felt my medical degree got shattered into pieces..
Fertility treatment..the other side of it
——————————————————-
Today the couple Mrs&Mr R came to me with their 6yrs old twin kids ,a male and a female.I remember to have referred this couple for higher level fertility treatment years back.The girl child was blind .The boy suffered Cerebral Palsy and was disabled physically and mentally.
Mrs R had conceived by the IVF Technic(Test Tube Pregnancy).They told me the third attempt at IVF only,succeeded.The couple were so highly elated at the TWIN conception that they could even forget their financial constraints.The treatment had incurred heavy expenditure.
The pregnancy period was a challenging one..She used to get small bouts of bleeding.She had to take absolute rest to avoid abortion.She had to undergo Cervical Encerclage (a stitch put around the lower end of the uterus to prevent preterm delivery).
In spite of all the efforts by her healthcare team and her own meticulous personal care the babies were born preterm (at the 27 th week of pregnancy) and weighed 600 and 650 grams.
The birth was in a centre where the Neonatology Department offered world-class facilities .The doctors assured 90% survival of the babies which was achieved too and the babies were live in front of me at their age of 6 years.
The miserable couple with the helpless invalid kids provoked my mind.Why were they made to survive? But many other babes born extremely preterm like these survive without any morbidity. I myself being a Gynaecologist,can very well understand how sincerely such babies are cared for in our technically perfect institutions.I know their success stories personally.I am never against advanced infertility treatment extended to the needy couples.
The inevitable happens to the ill-fated ones.Food for thought…